Ankle Ligament Injury
High Ankle Sprain
Read More >

Minute Read
|Posted 4 years ago
|Last updated: 10/10/2023
|by James McCormack

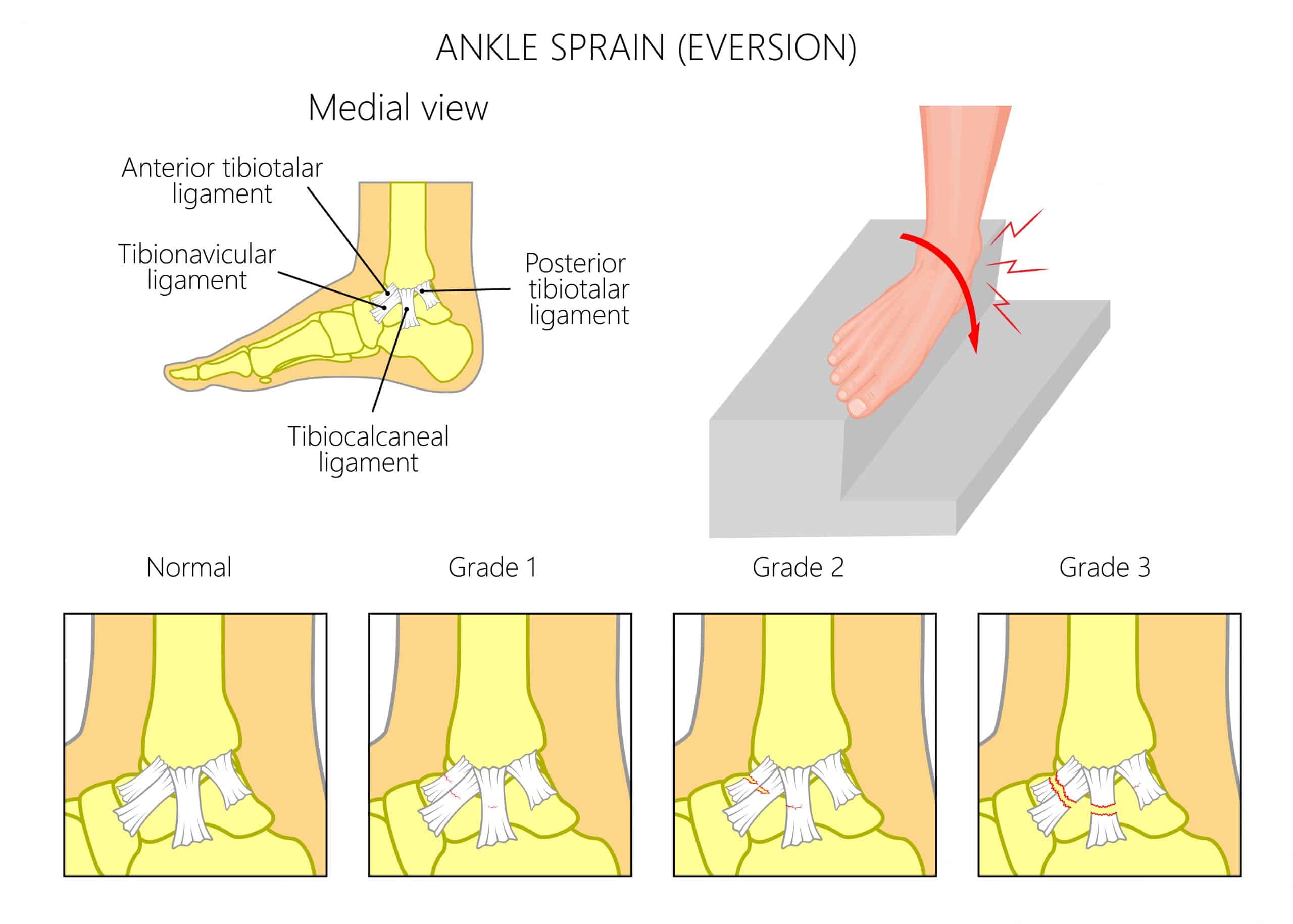
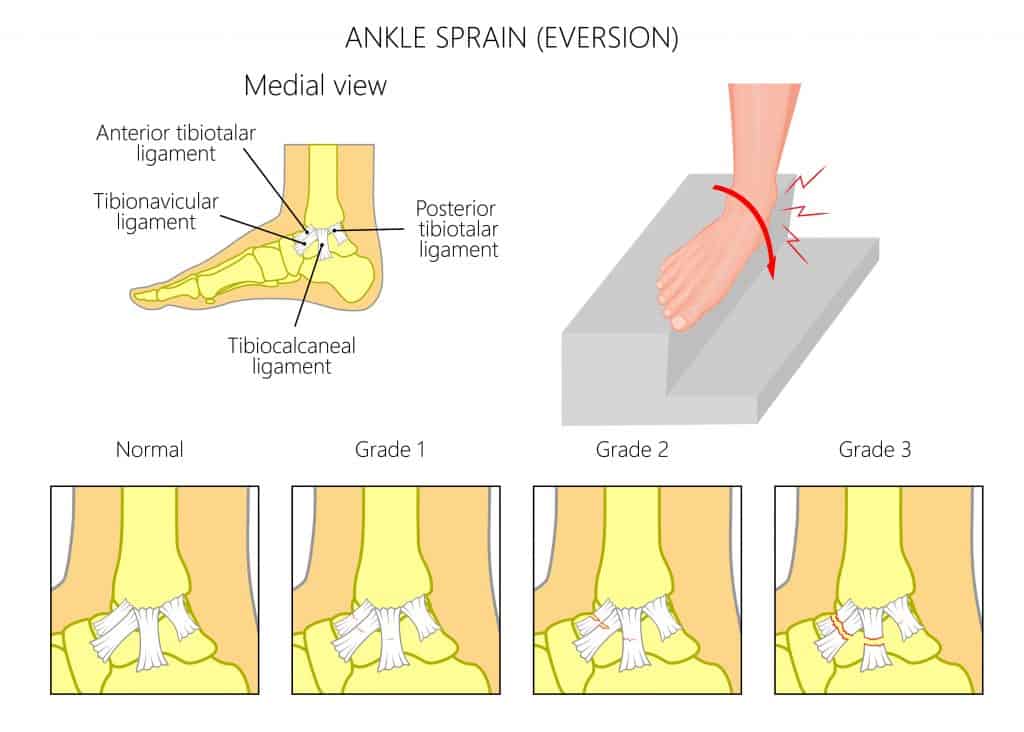
The deltoid ligament sits on the inside of the ankle joint, connecting the medial malleolus (inner ankle bone) to the navicular bone on the arch of your foot, the calcaneus bone (Heel bone), and the talus bone. It is triangular in shape and consists of 4 ligaments that run across the inside of the ankle joint. There is an outer layer whose primary aim is to resist eversion (turning the ankle outwards), and the deep fibres act as a stabiliser of the talus bone.
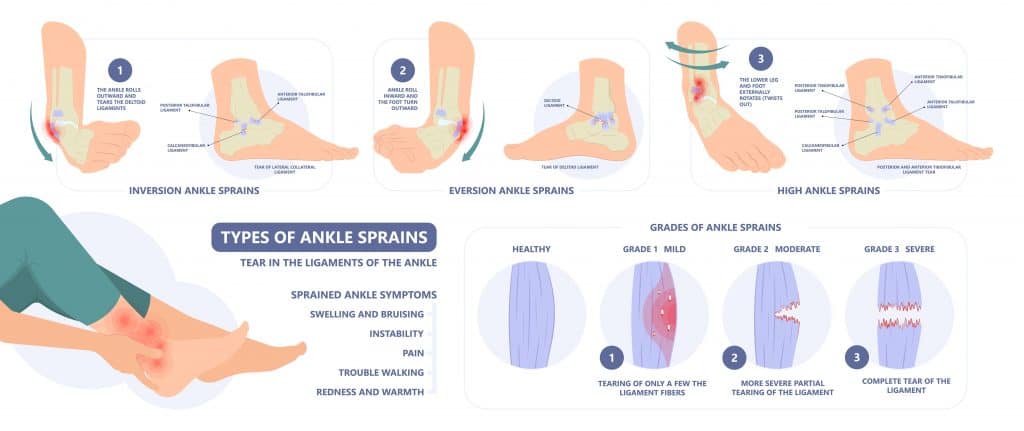
Deltoid Ligament Sprains, also known as medial ankle sprains, are much less common than lateral ankle ligament sprains. Up to 70% of the population incur an ankle sprain during their lifetime, and half of all ankle sprains occur during athletic activity. Medial ankle sprains account for approximately 15% of all ankle sprains.
One of the primary reasons that Deltoid Ligament Sprains are less common than the type of ankle sprains that occur on the outside of the ankle is due to the anatomical layout of the bones of the ankle. The bone structure supports the inner ankle joint, so while rare, they are painful and tricky to manage.
This article will explore the common causes and symptoms of Deltoid Ligament Ankle Sprains and how to treat them effectively. We have treatment protocols, information on healing times and what to do if your deltoid ligament sprain isn’t improving.
The deltoid ligament is a large fibrous ligament, and due to the articular shape of the medial ankle and the deltoid ligament, considerable force is required to cause injury.
Common mechanisms of injury are blunt trauma to the outside of the ankle that forces the ankle inwards, causing overstretching of the deltoid ligament. This may result from a tackle in a sport or from a fall.
Alternatively, foot deformity or poor biomechanics can overload the inner ankle and lead to repetitive strain on the deltoid ligament. This slow process occurs in conjunction with a weakening posterior tibialis muscle that progresses into adult flat foot deformity.
High-risk factors include quick change of directions in sports such as basketball, rugby, football and gymnastics.
Severe deltoid ligament sprains are often associated with high ankle sprains and dislocations or fractures.
Deltoid Ligament Ankle Sprains are often complex injuries. The location of the pain is on the inner ankle, with patients often describing a burning sensation.
There may be bruising and swelling when the outer fibres are torn, while there may be no visible signs of injury if the deep fibres are affected.
It is often painful to walk or rotate the ankle outwards. If the deep fibres are compromised, it may be painful to turn the ankle inwards.
In chronic medial ankle sprains, stiffness in the ankle joint can limit the range of movement available making it difficult to do activities such as climbing stairs and walking on uneven surfaces.
Up to 40% of ankle sprains still have residual symptoms after 6 months, highlighting the importance of prompt diagnosis and treatment.

Establishing a clinical diagnosis through a consultation with a Sports Medicine Doctor or a Physical Therapist is essential, as untreated medial ankle sprains can cause chronic symptoms.
After a clinical interview and physical assessment, a Physical Therapist may carry out a Klieger test to confirm their diagnosis.
A Klieger test requires the patient to be seated, with the knee hanging at 90 degrees and the ankle relaxed. One hand of the therapist stabilises the leg from behind; the other hand grasp the ankle in a neutral position, then externally rotates the foot. Medial ankle pain with laxity is a positive test.
In some cases, a referral for imaging may be required. An MRI is the gold-standard form of imaging for medial ankle sprains, as it can detect bony and ligament injuries. An ultrasound is a cost-effective alternative, while a CT Scan or X-ray cannot diagnose soft tissue injuries.
In the first three days of an acute Deltoid Ligament Ankle Sprain, it is best to apply the P.O.L.I.C.E principle, which stands for Protection, Optimal Loading, Ice, Compression, and Elevation and is a more effective form of management than the R.I.C.E protocol for this form of injury.
P.O.L.I.C.E involves offloading the injury area as much as possible. After three days, you can begin Optimally Loading the ankle within a pain-free zone or at least with movements that don’t worsen symptoms. Apply ice as an analgesic to help reduce pain levels and compress the ankle with a compression sock or bandage to minimise swelling.
The Optimal Loading phase is when Physical Therapy is most beneficial. Treatment may include ankle taping to reduce pain and facilitate a regular gait pattern. In more severe cases, you may require an ankle brace or walker boot to provide additional stability to the ankle joint.
We know that deltoid ligament sprains are likely to become stiff and chronic, so manual therapy such as deep tissue massage and mobilisations can be used alongside stretching exercises to restore ankle range of motion.
Rehabilitation will progress to more challenging strengthening, dynamic proprioception, and plyometric exercises. An exercise protocol involving theraband exercises, bodyweight strengthening, and balance exercises are beneficial in the early stages of rehabilitation. A Physical therapist may provide soft tissue massage and mobilisations to help restore the range of movement to the ankle.
The final stages of rehabilitation involve a change of direction in exercises and returning to running or sports protocols. This stage is often completed without the need for taping or ankle support.

A steroid injection may be advised if pain levels are too high to tolerate rehabilitation. The purpose of an ultrasound-guided injection to the medial ankle joint is to reduce inflammation levels. This is a more common treatment for tears of the deeper fibres, but some risks are involved, such as a steroid flare or infection.
Surgery is rarely recommended for Deltoid Ligament Ankle Sprain, even if it is a Grade 3 rupture. This is due to the articulation of the medial ankle joint providing natural stability to the joint. In the cases of surgery, a cadaver ligament is often used. Surgical cases often involve ankle joint disruption, including ankle dislocations and high ankle sprains. After surgery, you may require time in a boot or cast before beginning ankle rehabilitation.
Grade 1 Deltoid Ligament sprains can recover within 2 weeks if they begin rehabilitation immediately under a physical therapist’s guidance. In most cases, it takes 4-6 weeks for a Grade 2 Deltoid Ligament Ankle Sprain to heal, while severe sprains of the deltoid ligament can take 12 weeks to recover.
You must carry out comprehensive treatment for this condition. Normally in the latter stages of recovery, it can feel like your ankle is back to normal, but this is the most important part of rehabilitation for reducing your risk of injury recurrence.
Evidence suggests that carrying out warm-up exercises can increase neuromuscular control and reduce the risk of ankle sprains while having the correct footwear can reduce your risk of an ankle sprain.
Regular ankle sprain exercises can increase neuromuscular control, strength and flexibility to reduce your risk of re-injury.
In mild cases, it is possible to return to linear non-impact activities such as static cycling and swimming within the first few days of injury. If there is no pain while doing exercises, continuing with this when you have a Deltoid Ligament Ankle Sprain is generally okay. However, consulting a healthcare professional before starting any exercise program is essential.
Yes, a deltoid ligament can be repaired surgically. A repair is usually done with a cadaver ligament, but it is a complex surgery with a lengthy recovery phase afterwards. Surgery is only recommended in severe cases or when conservative management has failed.
This article is written by James McCormack, a Foot and Ankle Specialist who is an expert in treating a Deltoid Ligament Sprain.
This is not medical advice. We recommend a consultation with a medical professional such as James McCormack if you are experiencing any of the symptoms discussed in this article. James offers Online Physiotherapy Appointments weekly and face-to-face appointments in his London clinic.