Braces and Supports
Brace for Runners Knee
Read More >

Minute Read
|Posted 4 years ago
|Last updated: 30/11/2023
|by James McCormack

Known as ‘Runners Knee‘ or PFPS, patellofemoral pain syndrome is a painful condition that affects the front of the knee. Specifically the patellofemoral joint between the knee cap and the femur. Pain is generally felt behind the kneecap but can be more vague anterior knee pain.
It is common among runners, hence the name. But can be caused by any activity which repeatedly bends and straightens the knee. This includes squatting, cycling or using a clutch when driving or prolonged sitting with a bent knee.
The two groups that are most likely to get PFJP are amateur runners and new military recruits. This is due to a change or increased use of the knee. And, possibly due to poor strength and conditioning.
There is a higher risk for women than men and it is more common in adolescents than adults.
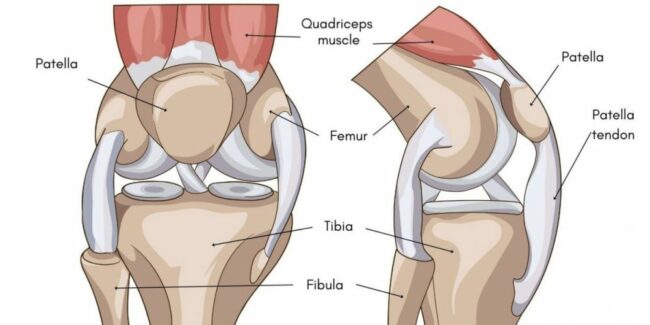
The knee joint comprises two weight-bearing bones, the tibia and the femur. A third bone, the patella (kneecap) is none weightbearing.
The patella sits in the quadriceps tendon. It is in contact with the femur bone, and this contact surface and pressure changes as the knee is bent and straightened.
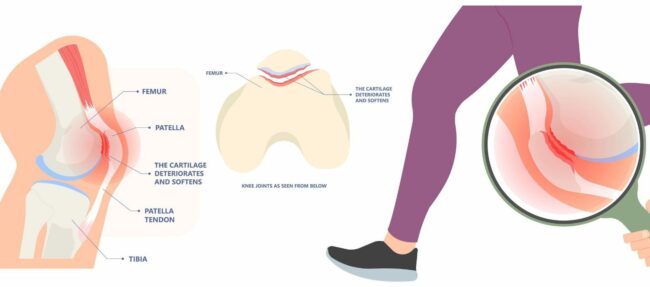
The back of the patella is covered with 4-5mm thick cartilage. This protects it against the contact, compression and friction of the femur during movement. Patellofemoral joint pain is irritation of the underside of the patella.
The patella acts like a pulley over the knee and improves the function of the quadriceps muscle. It also protects the quadriceps tendon, which would otherwise have high compression and friction with each knee bend.
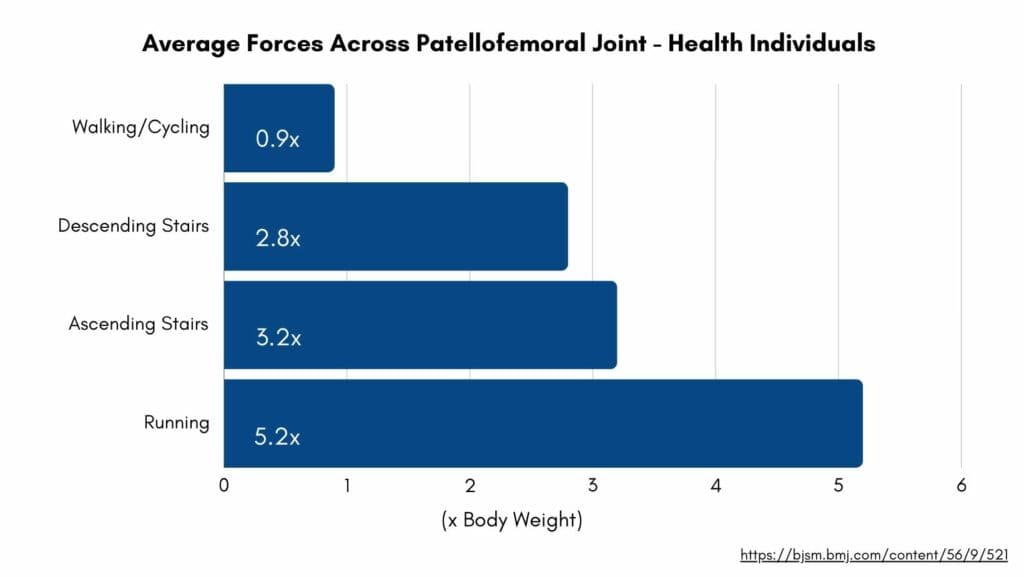
Between the angle of 60-90º knee bend, the patella has the greatest contact with the femur and sits firmly in the intercondylar groove. The forces across the patellofemoral joint, therefore, are affected by the angle, weight and impact of the activity.
As the knee bends, the contact area of the patella on the femur also changes. The further the knee bends, the closer the contact is to the top of the patella. The straighter the knee the lower down the contact point is.
Runner’s knee is commonly described as a feeling of pain underneath or behind the kneecap. It can affect one or both knees. Pain is typically felt with activities such as walking, running, walking down stairs or walking downhill.
It can also be felt when sitting when the knee is bent. Pain can last for several hours or days after the aggravating activity. The duration will vary depending on several factors: pain severity, duration and the condition of the patellofemoral joint.
A common complaint is stiffness or clicking of the joint as well as pain. These sounds are described as crepitus.
The knee might feel stuck or locked in particular positions in more severe cases. Many people say they need to move the knee through that position to click the knee, and it will feel like it has been released.
Pain can be severe to prevent walking and sleeping.
An irritation to the patellofemoral joint causes Runner’s knee pain. This can be caused by repeated irritation, such as running. Or by a sudden overload to the joint, such as from the trauma of a fall onto the knee. Or can be an insidious onset with no known cause.
Some activities put high stress levels and load through the patellofemoral joint, such as running, jumping and squatting. And and individual’s biomechanics when doing these activities will influence their risk.
Specific biomechanics have a greater risk of developing this condition. Risk factors include:


Discussing recent changes in activity or the mechanism of injury can reveal overload to the patellofemoral joint. A thorough physical examination will look at movement patterns and symptoms with movement will clarify.
A commonly used cluster of clinical tests is below with 2/3 being positive to indicate a diagnosis of Runner’s Knee:
If there is uncertainty about the diagnosis or if symptoms are not improving in the expected time frame, then additional information from imaging may be useful. An X-ray can rule out bony injury or an MRI can show inflammation or damage to the back of the patella.
With a prompt and accurate diagnosis, and correct management the healing time for Runner’s knee is typically 4-6 weeks. Some rehabilitation exercises require tolerating low pain, which should be monitored. However, pain caused by activities that do not improve strength or flexibility should be avoided as much as possible.
Relative rest is effective. That is resting from or reducing the volume or intensity of aggravating activities but keeping active and working on specific rehab exercises.
Physical therapy can help recovery from Runner’s knee with massage, advice and rehab exercises.
Massage, stretching and foam rolling will be the most effective in the early and most painful stages. In many cases of patellofemoral pain syndrome, tightness of the quadriceps muscle, specifically the lateral part, can play a significant role in this condition’s development or persistence.
Assessing the biomechanics of an individual with different movements will guide what specific exercises will be helpful. Rehabilitation exercises should focus on your specific needs.

Surgery and other invasive interventions, such as injections, are rarely necessary and not always effective for the treatment of patellofemoral pain syndrome. Only in extreme cases of patella malalignment might surgery be offered.
Physiotherapy with James McCormack
This article is written by James McCormack, a Lower Limb Specialist who is an expert in treating Knee pain.
This is not medical advice. We recommend a consultation with a medical professional such as James McCormack if you are experiencing any of the symptoms discussed in this article. James offers Online Physiotherapy Appointments weekly and face-to-face appointments in his London clinic.