Ankle Bone or Joint Injury
Anterior Ankle Impingement
Read More >

Minute Read
|Posted 3 years ago
|Last updated: 03/12/2022
|by James McCormack

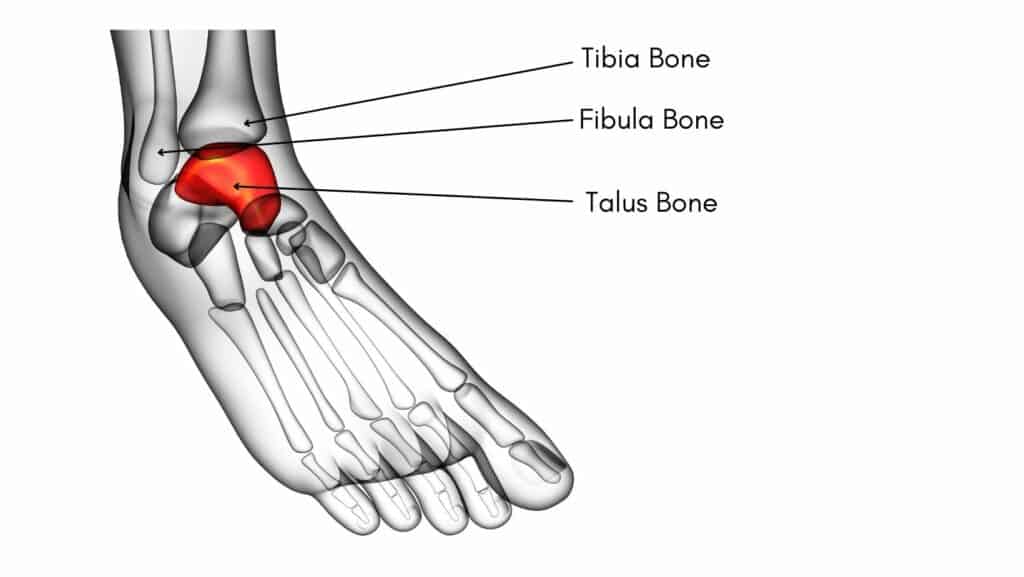
The Talus bone is an irregular-shaped bone with a neck and oval head. It is also known as the ankle bone as it sits between the Tibia, Fibula and Calcaneus. The Talus is the second largest tarsal bone and has the highest percentage of cartilage cover of any bone in the body. Cartilage is a strong protective substance that surrounds the end of each bone to protect it.
The Talus plays a vital role in weight-bearing activities, providing structural stability to the ankle joint, although unlike most bones in the body, it has no muscular attachments. Due to the high levels of bony articulations around the Talus bone, it is likely to develop changes to its cartilage if excessive pressure is placed on it. In these instances, a small area of cartilage can break down on the Talar Dome, and this is known as an Osteochondral Lesion of the Talus or Osteochondritis Dissecans.

An Osteochondral Lesion of Talar Dome causes pain in the front of the ankle joint, or patients often describe a deep aching pain in the ankle joint that they are unable to touch. Symptoms are often worse with activities such as running, walking uphill or on uneven surfaces. Patients may describe a locking or clicking sensation, which is often due to a loose cartilage fragment becoming caught between surfaces. There are often mild levels of swelling associated with this type of injury.
Symptoms are generally worse with activity but improve with rest, while less supportive footwear can irritate the symptoms of an Osteochondral Lesion of Talar Dome. There is often a reduced range of ankle motion with pain during a heel-over-toe exercise.
One of the most common causes of an Osteochondral Lesion of Talar Dome is a moderate to severely sprained ankle. The rotation element of the injury can cause friction between the chondral surfaces and result in an Osteochondral lesion.
Repetitive strain or impact from activities such as running can cause a slow deterioration of the cartilage if there is excessive strain on one aspect of the talar dome biomechanically. A high arch or pes cavus foot type can put you at a slightly high risk of developing an Osteochondral Lesion of the Talar Dome.


There is no specific test to identify an Osteochondral Lesion of the Talar Dome, clinically. A Physical Therapist can carry out an Anterior Ankle Impingement test to identify an issue at the front of the ankle. Still, it doesn’t differentiate between an Osteochondral Lesion of the Talar Dome and a bone sport or soft tissue impingement. An x-ray is usually requested if you have the symptoms of an Osteochondral Lesion of the Talar Dome, which is easily accessible and cheap. If an Osteochondral Lesion of the Talar Dome is confirmed by x-ray, then an MRI may be requested to identify the size and location of the lesion.
In cases where there is an Osteochondral Lesion of the Talar Dome that is small and especially in a younger population, conservative treatment is highly effective for this condition as regeneration of the area around the lesion is possible. Treatment can involve using a walker boot for 4-6 weeks to reduce inflammation around the lesion and allow it to heal. Using anti-inflammatories in the initial 2 weeks post-injury can be beneficial. Walking is generally permitted for short distances within the boot as pain allows.
Once the walker boot is removed, Physical Therapy should commence immediately, consisting of balance, stretching and strengthening exercises. An ankle brace may be recommended to support the foot. In addition, weakness of the foot and ankle from wearing the boot needs to be addressed, and a gait analysis should be carried out to identify any biomechanical factors that may have caused the initial injury.

Insoles may be required to provide additional support to the foot or in some cases, stability trainers may be sufficient. A thorough return to sport protocol should be developed, especially if the individual wishes to return to impact or change of direction sports.
If conservative treatment for an Osteochondral Lesion of the Talar Dome is unsuccessful then surgery may be considered. Surgery may be in the form of an arthroscopic procedure where the joint is cleaned and shaved around the lesion or a microfracture of the lesion to encourage new cartilage formation in the affected area. These treatments have mixed outcomes and we recommend exhausting all conservative measures before considering surgical procedures.
This is not medical advice. We recommend a consultation with a medical professional such as James McCormack. He offers Online Physiotherapy Appointments for £45.
Related Article: Anterior Ankle Impingement: Symptoms & Treatment