Foot Exercises
Hallux Rigidus Exercises
Read More >

Minute Read
|Posted 4 years ago
|Last updated: 14/11/2023
|by James McCormack

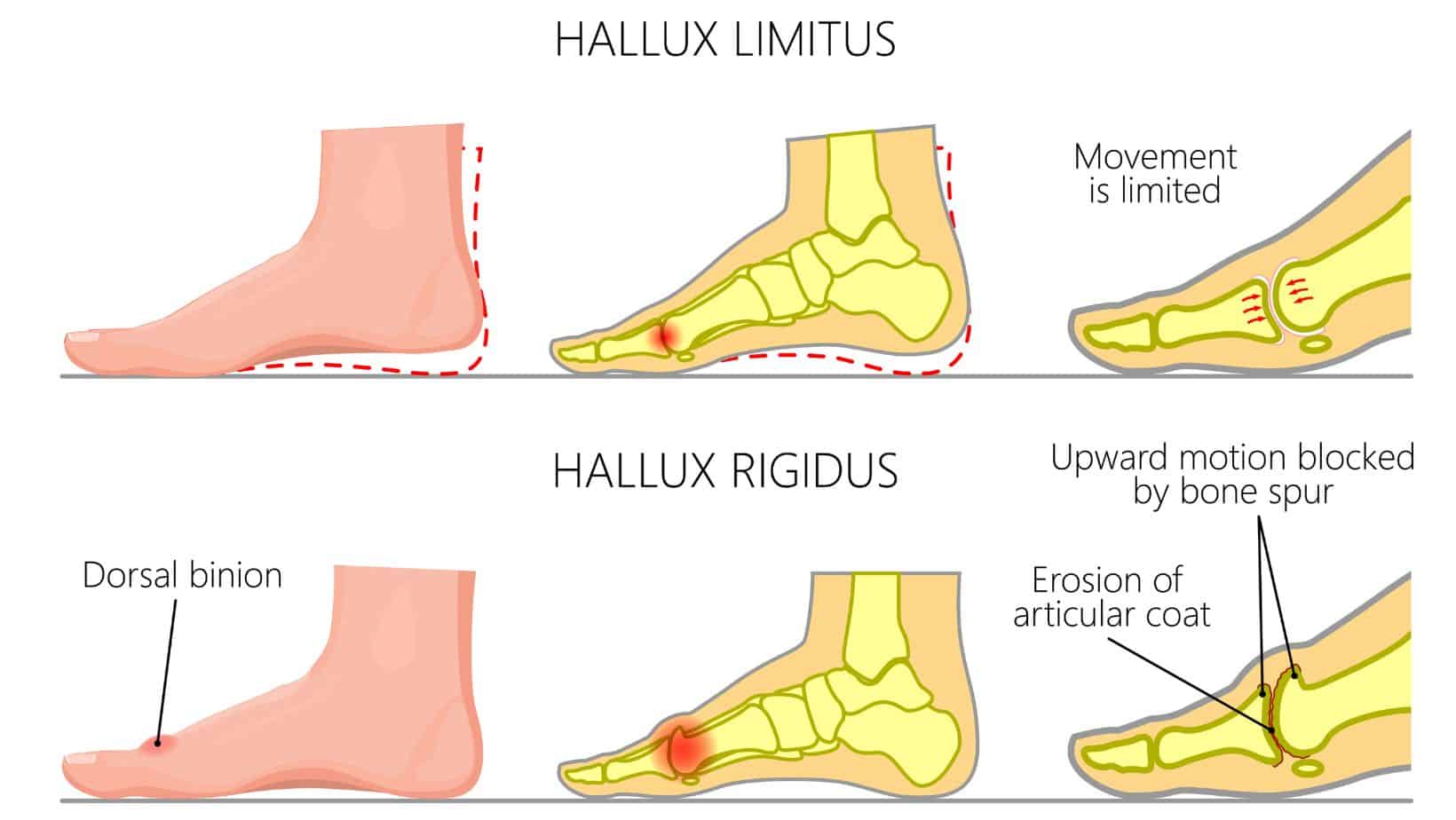
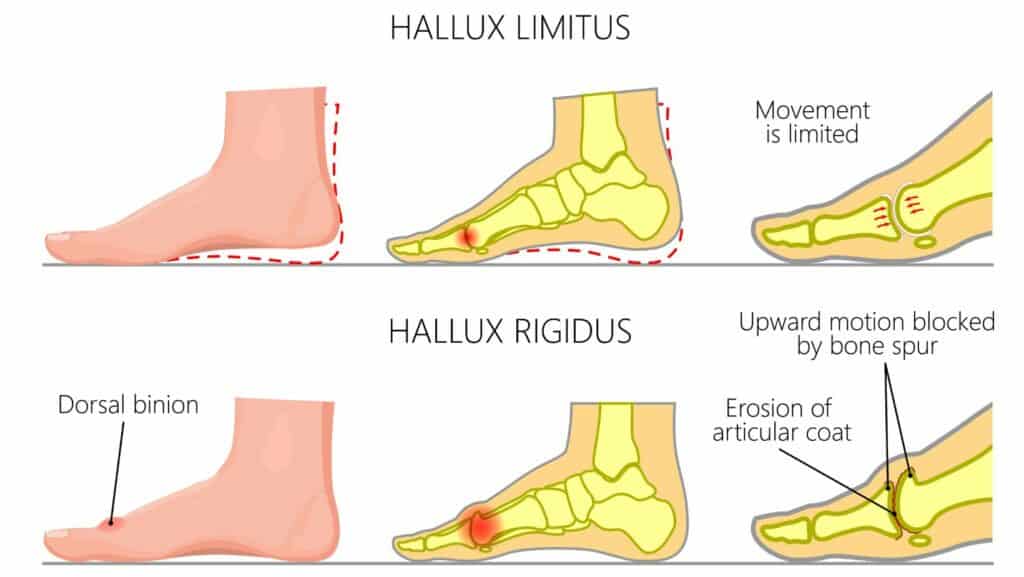
Hallux Rigidus and Hallux Limitus are conditions that affect the big toe joint. Hallux Limitus result in a restricted range of motion in the big toe joint from soft tissue tightness, whereas Hallux Rigidus is a painful big toe joint that results from big toe arthritis.
For normal mechanics for the big toe, 65-75º of dorsiflexion of the hallux on the 1st MTP is required. During this process, the 1st ray is required to plantarflex through contraction of the Peroneus Longus by pulling on a stable longitudinal arch of the foot. Soft tissue tightness can contribute to a reduced range of motion at the 1st MTP, while osteophytes, arthritis or osteochondral lesions can significantly limit the range of motion.
Hallux Rigidus affects up to 2.5% of the population over 50, and it is twice as common in females as males. Hallux Rigidus can significantly affect ones quality of life as the 1st metatarsal transfers approximately 119% of one’s body weight through the gait cycle. If this movement is limited, it can cause pain, reduced function and well-being.
The symptoms of Hallux Rigidus include pain and stiffness when extending the big toe, primarily felt when walking, running or going up onto your tip toes. The joint can be visually red, hot to the touch and swollen. Like most degenerative arthritis conditions, patients find the symptoms exacerbated in colder weather.
As symptoms of Hallux Rigidus deteriorate, there may be pain at rest, numbness and a complete inability to bend your big toe joint. Numbness can be caused by a bone spur impinging a local nerve while exercises such as lunges and running can be too painful. Wearing tight-fitting shoes or high heels can be exacerbated the symptoms of Hallux Rigidus, while a shallow toe box can be painful for those with a dorsal osteophyte.
Patients with hereditary Hallux Rigidus may not have any pain; it may be years before they notice the condition.
Patients can develop Hallux Rigidus insidiously over time, with speculation that it results from a subtle biomechanical overload over a long period. Those with jobs that involve a lot of squatting or bending down can be more susceptible to developing Hallux Rigidus.
Structural abnormalities of the foot, such as having a flat foot, can overload the big toe joint, leading to arthritic change within the MTP joint. In contrast, poorly fitted shoes or high heels can similarly affect the joint.
Direct impact or a fracture to the big toe joint can accelerate the rate of arthritic change within the joint. At the same time, other factors, such as rheumatoid arthritis or gout, can make you more susceptible to developing Hallux Rigidus.
Hallux Rigidus is more prominent in females and approximately 80% of patients with bilateral Hallux Rigidus had a family history of big toe arthritis or bunions (hallux valgus)

A Physical Therapist or Podiatrist is in an excellent position to clinically diagnose Hallux Rigidus as it is easily identifiable through a Physical Examination. Clinically, we can expect an altered gait with greater lateral loading of the forefoot and an early heel lift to compensate for the lack of 1st MTP extension. The affected foot should be assessed in standing and laying to establish the hallux’s passive and active range of motion.
If the clinician wants further information on the condition’s severity, they may refer a patient for imaging. An X-ray is the normal first port of call as it is cheap and can accurately identify any loss of joint space and osteophytes (bone spurs).
A clinician may request an MRI or CT scan for a more detailed image of the foot, including soft tissue structures and information on swelling that an X-ray does not.
Home remedies are usual for the initial management of Hallux Rigidus, including regular icing and taking anti-inflammatories. Physical Therapy is an excellent approach to managing this condition; seeking a therapist who regularly sees foot conditions is essential. A physical examination should reveal imbalances in foot mechanics that can be addressed with strengthening and stretching exercises.
In some cases, custom insoles or orthotics may be recommended, with the purpose being to limit the range of motion in the big toe, usually with Morton’s extension, as this can provide pain relief. Discussing with your clinician about footwear is essential as a shoe with a large toe box can relieve pain, while a trainer with a rocker bottom sole is also beneficial.
A brace, taping, massage and joint mobalisations are all effective short-term pain relief, but ultimately, footwear, orthotics and exercises are the best forms of treatment for Hallux Rigidus.
If a patient tries these methods but continues to struggle with pain levels, a corticosteroid injection may be provided as this provides steroidal anti-inflammatories directly into the joint, providing 6-12 weeks of pain relief to recommence Physical Therapy.

Unfortunately, for severe cases of Hallux Rigidus, surgery is the only viable option due to the considerable changes within the joint space. The most common surgeries for Hallux Rigidus are as follows:
Cheilectomy: A cheilectomy is an arthroscopic procedure where bone spurs are shaved off to provide pain relief and preserve the joint
Osteotomy: An Osteotomy involves shaving or cutting the bone to realign it
Arthrodesis: Arthrodesis is a fixation of the bones using plates, screws or wires to stop the joint from moving and is used primarily for severe cases.
Arthroplasty: An Arthroplasty is the artificial replacement of one or both ends of the joint with a plastic or metal replacement
In our experience, if you have Hallux Rigidus but no symptoms, you can continue running.
Suppose you have no pain when running but mild pain afterwards. In that case, we recommend continuing to run while ensuring you have the optimal footwear and seeing a Physical Therapist for mobility and strengthening exercises.
If you have constant pain that worsens when running, we recommend you stop and see a foot specialist for a consultation.
This article is written by James McCormack, a Lower Limb Specialist who is an expert in treating Hallux Rigidus.
This is not medical advice. We recommend a consultation with a medical professional such as James McCormack if you are experiencing any of the symptoms discussed in this article. James offers Online Physiotherapy Appointments weekly and face-to-face appointments in his London clinic.