Foot Bone or Joint Injury
Cuboid Syndrome
Read More >

Minute Read
|Posted 4 years ago
|Last updated: 27/03/2023
|by James McCormack

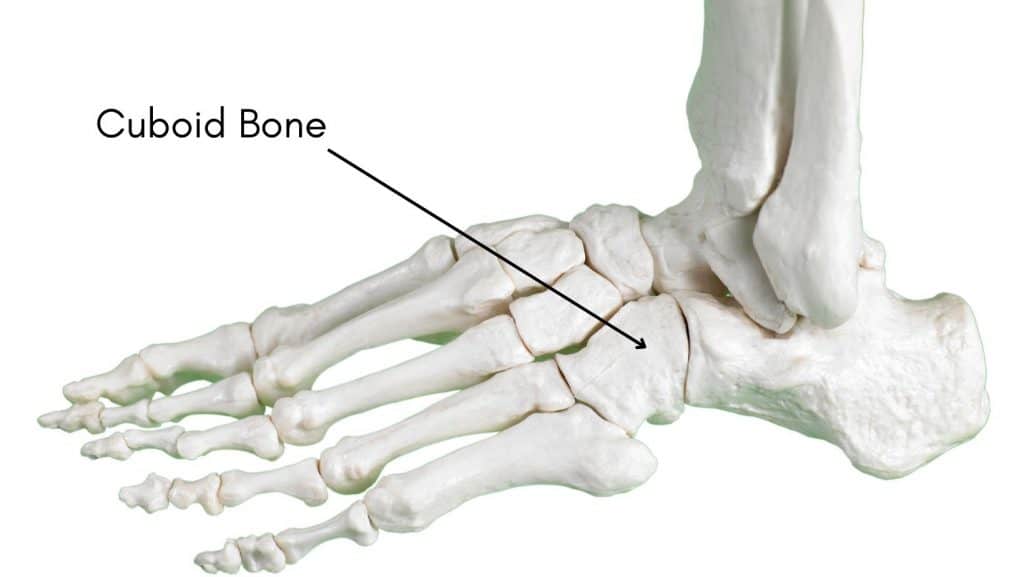
The cuboid sits on the outer aspect of the foot, and it is one of seven bones in the foot. It is cube-like in shape, sitting behind the 5th metatarsal and in front of the calcaneus. The cuboid bone plays a significant role in the dorsiflexion and plantarflexion of the foot while also being involved in pronation moments of the calcaneocuboid joint.
During the gait cycle, the cuboid bone alongside the Peroneus Longus muscle help to stabilise the foot’s lateral column to prevent excessive pronation forces.
The annual incidence of cuboid fractures is 1.8 injuries per 100,000 population which is quite low compared to calcaneus fractures, approximately 11 per 100,000 people per year.
The cuboid bone articulates with four bones of the foot:
There are 5 main classifications of cuboid fractures that we have outlined below:
An avulsion fracture is where a tendon or ligament pulls off a fragment of bone.
A stable isolated extra-articular fracture. This does not need surgery
These are stable, intra-articular fractures and are managed conservatively.
These are associated with disruption to the midfoot alongside tarsometatarsal injuries.
This involves a crushing injury of the cuboid that can be accompanied by disruption to the mid-tarsal joint and the lateral and medial column. Sometimes these are treated conservatively but primarily by surgery.
Cuboid fractures present with symptoms of pain on the outside of the foot just above the 5th metatarsal.
There can be pain on tip-toe walking, running or hopping that can be sharp and immediate in onset.
There may be swelling and bruising on the outer foot.
The patient often avoids walking on the outer aspect of their foot.


Clinically, there is often tenderness on direct palpation of the cuboid over the lateral aspect of the midfoot, while the fracture can be accompanied by deformity, ecchymosis, or fracture blisters.
A conventional x-ray is recommended initially for a suspected cuboid fracture. Still, these are only up to 35% sensitive in the early stages of injury, rising to 70% if scanned 2-3 weeks post-injury.
An MRI is often used to confirm a diagnosis. If an x-ray or MRI indicates a cuboid fracture, a CT Scan may be necessary to establish the severity and classification of the fracture.
Most types of Cuboid Fracture are treated conservatively under a Physical Therapist’s care. A conservative protocol typically involves 4-6 weeks in a walker boot, with the first 2 weeks partial weight-bearing before progressing to full weight-bearing.
A therapist may perform gentle calf massage to maintain calf length and ankle mobilisations to maintain mobility within the foot and ankle.
When the boot is removed, a graded strengthening, mobility and stability programme commences ensuring full recovery with no secondary complications.
Surgery is rarely recommended, and the cases that require surgery typically type 5 fractures with at least 1mm of displacement. Surgery can involve an ORIF with or without bone grafting.
It takes 6 weeks for a Cuboid fracture to heal in a walker boot and an extra 6 weeks of rehabilitation with a Physical Therapist for complete recovery from a cuboid fracture so 12 weeks in total.
You can walk short distances of 10-15 minutes in a walker boot with a cuboid fracture. The pain levels should dictate the time or distance; if pain levels increase, you should consider less walking or using an aid such as crutches to reduce the weight placed through the foot.
This is not medical advice. We recommend a consultation with a medical professional such as James McCormack. He offers Online Physiotherapy Appointments.
Other causes of Outer Foot Pain
Cuboid Syndrome – Peroneal Tendon Tear – 5th Metatarsal Fracture