
Braces and Supports
ACL Braces
Read More >

Minute Read
|Posted 4 years ago
|Last updated: 20/11/2023
|by James McCormack

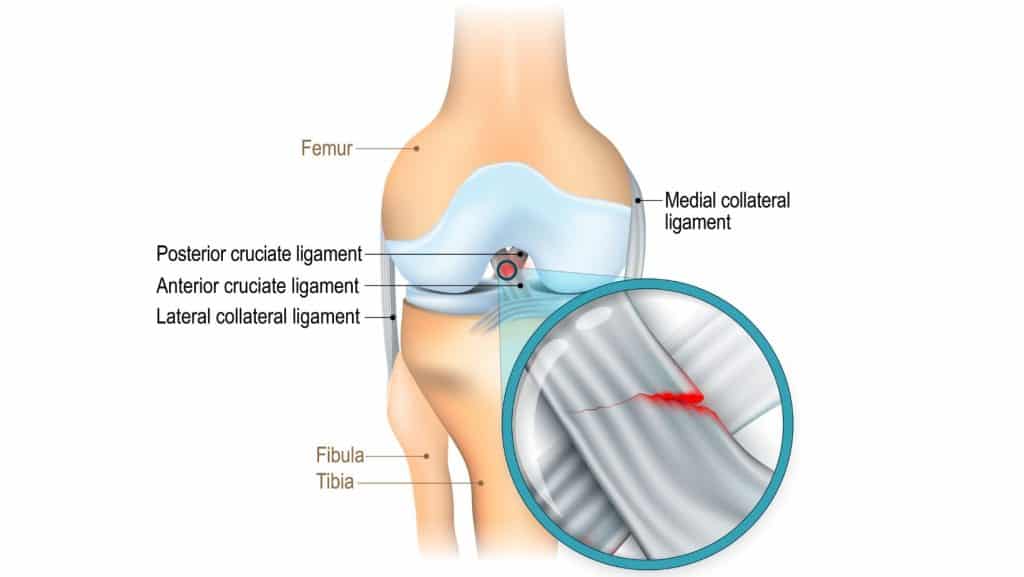
The ACL is the anterior cruciate ligament of the knee. It is attached to the bottom of the femur and runs diagonally forward to insert into the tibia. This diagonal direction means the ACL can control and restrict the forward movement of the shin relative to the femur.
There is a second cruciate ligament, the PCL, or posterior cruciate ligament, which is similar to the ACL but runs diagonally backwards from the femur to the tibia and has the opposite function of restricting and controlling the backward movement of the tibia relative to the femur.
Ligaments are thick, strong tissue made of collagen. Their primary role is restricting unwanted movements in a joint and to allow for efficient movement in the desired planes. They also have a secondary role, proprioception, and they can give feedback to the brain about the movement and position of the knee. This information is valuable as the brain can then send signals to the body’s muscles to correct positions to keep up balance and upright and move efficiently to prevent injury.
An injury can be a stretch or tear of the ligament. The extent of stretch or the percentage of fibres torn, or the type of tear will influence the extent of the functional compromise.
Ligament injuries are diagnosed as grade 1-3 depending on the laxity and percentage of fibres torn. The ACL is one of the most commonly injured ligaments of the knee.
Injuries of the ACL often also involve injury to another structure in the knee; a tear of the meniscus or medial collateral ligament is the most common.
An ACL tear is often referred to as a pivot shift injury due to the mechanism that causes this injury. The ACL is most stressed and vulnerable to injury with sudden changes in speed or direction.
Significantly slowing down or suddenly stopping, landing awkwardly on your knee, pivoting on your knee when your foot is fixed, or a direct impact to the side of the knee like when players collide in a tackle.
When an ACL tear occurs, many people report a popping or cracking sensation and other symptoms, such as significant swelling, within several hours.
The swelling will make it difficult to bend or straighten the knee fully. It is often painful to bear weight on the injured leg, and it is impossible to continue playing sport.
In some cases, a feeling of instability is also noticed. Pain may be much lower with a mild injury, but the feeling of instability or that the leg might give out can be felt. In some instances, swelling can be so significant it can distort the feeling of instability.
The instability can vary from feeling very vulnerable with any movement to more subtle and only felt with movements that stress the injured ACL. These movements include jumping and landing, rapid deceleration, quick direction changes or pivoting on the knee.
As time passes, the later symptoms will be noticed. Bruising can often take several days to appear and can be significant in some injuries.

See a medical professional if you suspect you have injured your ACL, such as a sports doctor or physical therapist. They will be able to examine your knee and recommend any additional diagnostics such as MRI or X-Ray that can confirm the diagnosis. Radiology such as MRI, is a very helpful to specifically diagnose the extent of the injury and if other structures have been injured concurrently. Ligament tears are classified as grade 1-3 detailed below:
The ACL is stretched but not torn, so there will be no bruising
Typically there is low pain and slight swelling
The knee will not feel unstable unless the ACL is stressed specifically
On assessment the ACL will feel firm with no increase in laxity
The ACL is torn and there can be bleeding linked to this damage resulting in bruising
Pain may still be low or moderate but there can be more swelling
Function will be impaired so the knee will feel unstable
On assessment the ACL will have more laxity, but will still have a firm end feel
There can be pain with assessment and stress of the ACL
The ligament is significantly torn or completely ruptured, there will be bleeding so bruising will be come evident following the injury
Pain will still only be moderate in most people, but swelling can be extensive
Function will be severely impaired with the knee feeling very unstable
On assessment the ACL will have significant laxity and no end feel
The healing process of a torn ligament requires a blood supply to provide the elements needed for the repair. The blood supply to the ACL comes from a vascular synovial envelope, supplied from the genicular artery, that wraps around the ACL. The small blood vessels from this envelope link to a network of tiny vessels within the ligament (, 1983). When the ACL is injured and torn, this network of blood vessels is also damaged. Therefore, the blood supply will be compromised, the degree of which depends on the extent of the damage, and the healing will be impaired.
For this reason, the blood supply will be assessed in higher-grade tears, and surgery is often offered to an athletic population. This can be reconstructive or augmentation surgery, which will use a tissue graft, most commonly from the hamstring tendon, and sometimes the patella tendon or a donor graft.
There is a growing body of evidence to support a non-surgical approach to managing ACL ruptures.
The recovery time, with rehabilitation and without surgery, can take weeks or months, depending on the extent of the damage. A grade 1 typically will take 4-8 weeks, while a grade 2 tear will take about 3 months.
The recovery of the ACL depends on several factors, including the specific injury and extent of injury, the person’s activity levels, their fitness levels and their general health. In most cases, if the tear is assessed as minor enough that there is potential for it to repair itself, then rehabilitation with an experienced physical therapist will be the treatment offered.
Physiotherapy with James McCormack
This article is written by James McCormack, a Lower Limb Specialist who is an expert in treating knee ligament injuries.
This is not medical advice. We recommend a consultation with a medical professional such as James McCormack if you are experiencing any of the symptoms discussed in this article. James offers Online Physiotherapy Appointments weekly and face-to-face appointments in his London clinic.